 When talking about Parkinson’s, Michael J. Fox – I’m sure all of you know who he is! – is fond of saying, “Science is HARD!” And I totally agree with him – science, especially medical science, IS hard – between figuring out what a disease is, how it gets started, how it works, and then, hopefully, how to stop or cure it…. well, it’s way beyond what my little brain can do… Heck, figuring out that 2 + 2 = 4 is sometimes difficult for me, especially when I’m in a ‘Off‘ brain fog!
When talking about Parkinson’s, Michael J. Fox – I’m sure all of you know who he is! – is fond of saying, “Science is HARD!” And I totally agree with him – science, especially medical science, IS hard – between figuring out what a disease is, how it gets started, how it works, and then, hopefully, how to stop or cure it…. well, it’s way beyond what my little brain can do… Heck, figuring out that 2 + 2 = 4 is sometimes difficult for me, especially when I’m in a ‘Off‘ brain fog!
But bear with me, I got to thinking (uh oh, we’re in trouble now!) about us Parkie’s mainstream med, Levodopa – how it’s used, how it gets into the body, and why we are still, in 2021, getting ‘Off‘ periods. After mulling it over for awhile, I came up with what I think, anyway, is a possible answer. Now, it’s easy for me to say “I think this is what we should be looking at” and actually implementing the idea… But for today’s blog post I thought I’d run it by you, my readers, and get your thoughts on this idea. So here goes…
 Levadopa 101 (Again)
Levadopa 101 (Again)
Now, to understand where I’m going with this, you have to understand what Levodopa (or Sinemet as we Parkies refer to it) is, and how it works. So once again, let’s go back to Levodopa Class 101, and do a quick review.
Levodopa, discovered in the late 1960’s, is an amino acid structure. Once it enters a PD patient’s bloodstream, Levodopa – combined with Carbidopa (to help with nausea) – makes it’s way to the brain and is able to pass through the blood-brain barrier. Once inside, the brain does a little magic and synthesizes that Levodopa into dopamine, a neurotransmitter.
 Now, dopamine plays an important role in many basic functions of the brain, such as motor co-ordination, reward, and memory. Since a Parkie’s brain no longer produces an appropriate amount of dopamine (due to PD’s destructive effect upon the Substantia Nigra area of the brain, where dopamine is normally produced) we get the symptoms of Parkinson’s – tremor, rigidity, dystonia, slow movements, facial masking, and such. So, once that Levodopa is converted into dopamine, it increases the brain’s supply of dopamine, thus easing or sometimes even reversing our PD symptoms!
Now, dopamine plays an important role in many basic functions of the brain, such as motor co-ordination, reward, and memory. Since a Parkie’s brain no longer produces an appropriate amount of dopamine (due to PD’s destructive effect upon the Substantia Nigra area of the brain, where dopamine is normally produced) we get the symptoms of Parkinson’s – tremor, rigidity, dystonia, slow movements, facial masking, and such. So, once that Levodopa is converted into dopamine, it increases the brain’s supply of dopamine, thus easing or sometimes even reversing our PD symptoms!
Ah, if it only lasted. That’s one of the problems with Levodopa – once the brain goes through the extra dopamine, it again runs low and then our symptoms return. That’s why we have to take numerous Levodopa pills during the day, at regular intervals, to keep that dopamine flowing. And to make matters worse, as we progress in the disease and lose even, if not all, of our dopamine-producing cells in the Substantia Nigra, we end up taking more Sinemet pill at each dose, or take them more often. And that can then increase the risk of developing dyskinesia (another subject we won’t go into here today).
 Off Times This is one of those things that really plague us Parkies. An ‘OFF‘ time refers to when our meds run out or stop working before it’s time to take our next dose of Sinemet; whereas an ‘ON’ time refers to when our meds are working and the brain is getting what it needs of dopamine. These OFF times occur more often as we progress, and can occur on a regular schedule (like in the evenings); or, for some, can occur at any time during the day. Of course, when this happens, it results in our symptoms coming back in full force. Trust me, it’s no fun – especially if it’s an hour or longer till your next dose of Sinemet!
Off Times This is one of those things that really plague us Parkies. An ‘OFF‘ time refers to when our meds run out or stop working before it’s time to take our next dose of Sinemet; whereas an ‘ON’ time refers to when our meds are working and the brain is getting what it needs of dopamine. These OFF times occur more often as we progress, and can occur on a regular schedule (like in the evenings); or, for some, can occur at any time during the day. Of course, when this happens, it results in our symptoms coming back in full force. Trust me, it’s no fun – especially if it’s an hour or longer till your next dose of Sinemet!
 Take Yer Pills
Take Yer Pills
OK, enough Levodopa class 101; we’re almost at the point I can explain my idea or ‘answer‘. But one final thing we need to go over: How does Levodopa get into a Parkie’s body?
Well, the most common way is to – yep – take a pill; usually a tablet of Carbidopa and Levodopa combined (i.e. Sinemet). Now, once we take said pill, it is wrought with danger before it can even make it to our bloodstream. First, it takes time – it has to get through our gut and into the area between our stomach and the start of the small intestine called the duodenum. This is the ONLY place in the gut where Levodopa can be absorbed into the body – if it can’t make it there, or goes past that point, then our poor tired brain gets NO dopamine!
And there’s another danger awaiting that little pill of Sinemet – and that involves what you eat right before or after you take your med. That’s because – in the duodenum – not only is Levodopa absorbed, but also other nutrients from our food. In this case, protein. Protein and Levodopa compete to get absorbed – and in a lot of cases, protein wins, leaving Levodopa out in the cold! That’s why we are told to take our meds at least an hour before we eat. So let’s say we take our Sinemet and then right away eat one of Tom’s big ole turkey sandwiches (with bacon, of course), loaded with protein. If both the Sinemet and the sandwich arrive at the duodenum at the same time, more often than not the sandwich will get absorbed first – resulting in a delay of the Sinemet getting absorbed, if it even get’s absorbed at all! Hence, you get one of those wonderful OFF times we all love (yep, sarcasm).
 So, I’ll bet your now asking the question, “OK, Tom, I think I understand, and that stinks! There’s got to be an easier way! So, isn’t there a different and better method to get that Sinemet into your bloodstream?” And that, folks, is the proverbial question, of which I am going to try to answer: What’s really the BEST way to reliably and consistently get Levodopa into our bloodstream?
So, I’ll bet your now asking the question, “OK, Tom, I think I understand, and that stinks! There’s got to be an easier way! So, isn’t there a different and better method to get that Sinemet into your bloodstream?” And that, folks, is the proverbial question, of which I am going to try to answer: What’s really the BEST way to reliably and consistently get Levodopa into our bloodstream?
Well, you can’t just inject dopamine itself into your veins – I mean, I hate needles… Plus, pure dopamine can’t pass through the blood-brain barrier. So you’re left with having to use Levodopa instead. Now, those scientists and their related companies have come up with a few answers; although in my opinion, none of them are anywhere near perfect.
- First is an old favorite, SINEMET® CR, or Controlled Release. SINEMET® CR (carbidopa levodopa) is a sustained-release combination of carbidopa and levodopa. It was designed to release it’s contents (Levodopa) over a 4- to 6-hour period, rather than immediately. Although it’s been around for quite a while, it never really lived up to it’s hype. Even though it should work 4-6 hours between doses, it proved to be ‘unpredictable‘ in keeping level amounts of Levodopa in a patients bloodstream. It does work, and can help with off times, but it may not be consistent. Besides all that, it still has to go through the digestive tract, which means it is beset with the same issues as regular Sinemet. So, although it can be useful, it doesn’t solve the problem.
Direct Injection into Duodenum (Duodopa®). Duodopa is a gel mixture of levodopa and carbidopa administered throughout the day with a portable pump into the small intestine via a permanent tube that passes through the abdominal wall, the stomach and directly into the duodenum. This allows a constant amount of levodopa to be present in the blood, which can reduce motor fluctuations, and therefore decrease the number of times patients alternate between significant “off” time and uncontrolled movement (dyskinesia). However, IT DOES REQUIRE SURGERY! Now, I don’t want to offend any Duodopa patients out there – especially if it’s working fine for you – but I think of this as a “last gap” measure when everything else has failed. For the system to work, you have to carry a pump around with you; and as a verifiable “chicken” (Bawk Bawk), I can feel light-headed or faint at the sight of my own blood – and now they want me to have a tube running from my insides out? No thank you… and as with the previous solutions, I can’t consider it to be the best one – a niche solution? Yes, but not ‘best’ in my opinion.
Time-Released Levodopa (Rytary®). Released in 2015, Rytary is a capsule that contains both immediate and extended-release levodopa with carbidopa. In addition to lessening motor symptoms, Rytary may decrease total daily “off” time. With Rytary, you don’t take pills as many times during the day as you do with immediate release Sinemet; but you take MORE pills each time. Now, I’ve tried Rytary, and for me, it just didn’t work reliably. Sometimes it would work as it should; other times not; and still other times too much. Plus, since it is taken orally, it has the same issues with absorption and food as does regular Sinemet. So again, I can’t consider this a “best” solution.
Inhaled Levodopa (Inbrija®). I had been watching this medication and it’s clinical trials closely for a while, and their was a time when I may have considered this a ‘best‘ solution. Released in 2019, Inbrija is Levodopa you inhale into your lungs, designed to help treat the return of Parkinson’s symptoms between regular doses of medication. In a large clinical trial, Inbrija started improving motor symptoms in as soon as 10 minutes. Well, maybe this will work – it doesn’t go through the gut so won’t have any issues with food, and it starts working in 10 minutes? Wow! Unfortunately, I still can’t think of this as a practical or “best” solution… Why? Notice the underlined words above – “between regular doses…”. You see, Inbrija is designed as a ‘rescue inhaler‘, meaning it’s to be used if and when your pills don’t work. It was never intended to replace your pill form Levodopa, as you can only take a dose up to 5 times a day. Now, I actually use Inbrija to help me between med doses; it does help some, but it has a number of negatives (for me anyway)): (a) It’s incredibly expensive ($$$$); (b) I find that it doesn’t work as well as Levodopa (sometimes it doesn’t work at all!); (c) It only lasts about an hour; (d) I find it takes much longer than 10 minutes to kick on; and (e) Since it’s a powder, my lungs rebel the minute I inhale it – usually resulting with me having a coughing attack after the 5 seconds of ‘holding my breath‘ once you inhale the stuff. So yes, it is useful – I think more useful than most of the others – but because of the restrictions and side-effects, I can’t rate it the ‘best‘ solution.
- Others – There are other med solutions out there – things like APOKYN (an injection of the dopamine agonist apomorphine hydrochloride); Kynmobi (sublingual ‘under the tongue’ apomorphine); etc… but they too are not designed to replace pill-form Levodopa. So again, they don’t get my ‘best‘ solution rating.
Then of course, there is DBS (Deep Brain Stimulation). If you’ve been following my blog for any length of time, you know I am a proponent of DBS (I’ve had DBS surgery twice!) And although DBS can help reduce your intake of Sinemet, and help with your symptoms, it really isn’t a basis of figuring out a better way for the body to absorb Levodopa; so I am not considering DBS in this discussion.
 OK, So Now What?
OK, So Now What?
Questions so far? Yes, that little freckle-faced young lady in the back row…. “Well, Mr. Tom, we say again: It’s terrible that there isn’t currently a really good way to get your Levodopa… So what was the point in all this? What’s your idea??” Well, well, glad you asked!
Again, I will re-iterate that I am NOT a scientist – and it’s easy for me to think of a better Levodopa delivery system, but then trying to develop it and make it work… well, that’s the “hard” part of the science. But bear with me… So, after looking at all the current methods of getting Levodopa into the blood stream, I believe the best way to do it would be: TRANSDERMAL/SUBCUTANEOUS DRUG DELIVERY! “Trans…Sub.. what?” Well, that calls for one of Tom’s famous definitions:
Ah-Ha! Now you see (I think), but let me go further… The skin, being the largest organ of the human body (comprising roughly 10% of the body’s mass), can readily absorb different compounds. For thousands of years, we have placed substances (like lotions and ointments) on the skin for therapeutic effects and, in the modern era, a variety of topical formulations have been developed to treat local indications. There’s a difference, though, between this ‘topical‘ use, and the transdermal delivery of compounds. Transdermal formulations are designed to penetrate through the skin layer and exert their effects on deeper or more distant tissues; and can thereby be directly absorbed into a person’s bloodstream.
To date, most transdermal delivery systems for pharmaceuticals have been patches. One such transdermal product we should all be familiar with is the nicotine patches smokers use to help ‘kick the habit‘, so to speak. We Parkies actually have available a transdermal system called Neupro; in fact, I use this each day via a patch I place on my body in the morning! This, though, is a Dopamine AGONIST – NOT pure Levodopa. But using a transdermal delivery system for our Levodopa could have significant advantages over oral administration, such as: Minimal first-pass metabolism; Avoidance of the adverse gastrointestinal environment; and the ability to provide prolonged and controlled drug delivery. And since Levodopa can pass directly from the bloodstream to the brain, it supports using a transdermal-type approach.
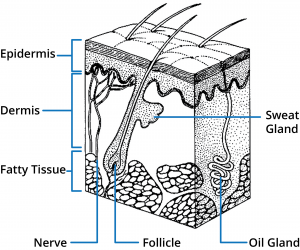
(Just as an FYI, here’s an image of what our skin looks like internally. I’m not going to go into how and where compounds get absorbed – you can find such info out on the web. Just trust me, it works and has been used before.)
Patches, by themselves, do not enhance the ability of a drug to permeate the skin but can increase drug absorption due to prolonged application times. However, this plain ‘patch‘ approach wouldn’t work well, with Levodopa. What we need is an ‘enhanced‘ patch – one with ‘microneedles‘. “Ugh, needles again!” you say. Hold on a moment – a microneedle is different than your typical intramuscular “shot in the arm” needle. Microneedles comprise arrays of micron-sized needles that offer a pain-free method of delivering compounds (like drugs) across the skin. Apart from being pain-free, microneedles provide various advantages over conventional vaccination routes such as the aforementioned intramuscular. By shrinking the needle to micron dimensions, we make use of its powerful delivery capabilities while improving patient compliance and safety.
 So how would it work?
So how would it work?
So using this technology, what do I envision in a device that we PD patients could use to best deliver Levodopa to our brains? Well, let me look into Tom’s crystal ball… I see a patch – thicker than the current patches like nicotine or Neupro – composed on the bottom of an array of microneedles. This part of the patch is what is place on your arm, thigh, or other area of the skin. On this patch would be a small pump – nothing like the pump used for Duodopa – but rather an integral part of the patch itself. Also on the patch would be a compartment that would hold a small container of sterile Levodopa; this container could be easily snapped in or out and replaced every day (or specific time interval) with a fresh new bottle. And, of course, a battery of some sort to run the pump and electronics.
The pump would slowly ‘inject‘, via the microneedles, the Levodopa in the container directly into the skin and thereby into the bloodstream. Thus, a patient would get a continuous supply of levodopa (amount determined by their neurologist) which should, in theory, maintain a consistent level of levodopa in the blood. Not only does this completely avoid all the gastrointestinal problems with oral pills, since it would maintain that constant level of Levodopa in he bloodstream, it should help with dyskinesia’s and OFF times! There could even be “smart” sensors on the patch that could sense and regulate the amount of drug delivered based upon that patient’s blood level!
And no, with the micronization of the needles and patch, I don’t envision the patch to be a huge thing or stick out like a sore thumb. It should be small enough to wear under a shirt, or on the leg. I can see, however, two problems with this approach:
- Skin Irritation: Using this patch might irritate the skin – either minimally or severely. However, I believe this could be avoided by routinely placing the patch at different parts of the body or skin… maybe one week on the arm; the following week on the thigh, etc.
- COST ($): In order to be useful to us Parkies, it would have to be priced so that we could AFFORD it on a regular basis! From what I’ve seen in the past, once new meds come out they are ridiculously priced – like Inbrija ($1,000/monthly w/o insurance) or even Neupro (over $700/month). I can only imagine what it would cost us for a system like this! But for me, however, the advantages of using a system like this might outweigh the cost… I may have to eat “Beans-N-Franks” for 2 weeks each month to afford the device, but it might just be worth it!
 What Tom’s Gizmo Might Look Like
What Tom’s Gizmo Might Look Like
So just what would a gizmo like this look like? Being an engineer (OK, Software Engineer) I think I can make an educated guess on its look and function. I first searched on the web, but was only able to find one design of what something like this might look like, and it’s below (and unfortunately no, I don’t know what the numbers represent)

OK, that looks kinda different… So here’s a pic of my design (remember, my only ‘F’ was in Art class, so no promises):
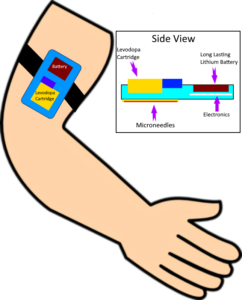
Well, as I said, I’m no artist, but I hope you get the picture. Levodopa itself really hasn’t changed much since it was discovered in the 1960’s; but it’s my personal belief that a system like this would revolutionize Levodopa delivery and create better and more stable lives for us PD patients.
Now, here is where the “I’m no scientist…” comes into play. Is this all feasible now?? In my little feeble mind, YES, it would seem to me that this could be designed for retail use. But that’s easy for me to say – someone (scientists and engineers) has to design it, get it to work, then run it through who-knows-how-many clinical trials to make sure it REALLY works for us Parkies and doesn’t cause any major side effects (like growing a third eye); then have it mass assembled, marketed, and finally sold into our hot little hands! That’s truly a lot of steps!! Having worked in the pharmaceutical and biotechnology fields for many years, I know how hard that is and how long it could take… But I relish the moment when I could have something like this available to me – ahhhh… the thought of much less OFF times with less dyskinesia makes me feel warm inside. But then I think of the time (and expense) of getting this developed and to market (and how much it’s gonna cost me!), and then that warm feeling turns into…. as Charlie Brown would say, “A big stomachache!” Seems like a hopeless case, at least in my lifetime, huh?
 But hold on – before we get all hopelessly whiney and depressed… Turns out that a device very similar to this is actually being worked on now!! A product, tagged ND0612, is currently in Phase III clinical development for Parkinson’s disease patients!
But hold on – before we get all hopelessly whiney and depressed… Turns out that a device very similar to this is actually being worked on now!! A product, tagged ND0612, is currently in Phase III clinical development for Parkinson’s disease patients!
Developed by a company called NeuroDerm, this investigational drug is designed to be continuously administered beneath the skin for 24 hours. The administration of ND0612 requires the use of a small pump, similar to the devices used to deliver insulin to people with diabetes.
They’ve developed two doses of ND0612: the low-dose (ND0612L) form is used to treat moderate stage Parkinson’s patients who can no longer effectively control their motor complications with oral levodopa, and a higher dose (ND0612H) for the treatment of severe Parkinson’s patients for whom oral drugs are no longer effective. ND0612 was designed to be a safer, more effective and convenient alternative to surgical treatments. Sounds a little bit like my gizmo, huh?
For those interested, the clinical trial (called BouNDless) is, I believe, recruiting participants for the study. To see if you qualify, go to their website and fill out the “Pre-Qualify” questionnaire. (Unfortunately, for those of us who have undergone DBS surgery – alas, we are NOT qualified!) Remember, participating in a clinical trial helps all us Parkies since it (hopefully) speeds up the process of testing and approval of new drugs and devices.
 So there you have my idea – whether it is feasible or not waits to be seen – but at least something similar is currently being worked on. Hopefully someday in the next few years it might be available to us Parkinson’s patients, and I relly think it will help us enjoy our lives even better. Now that is news to be hopeful for, huh?
So there you have my idea – whether it is feasible or not waits to be seen – but at least something similar is currently being worked on. Hopefully someday in the next few years it might be available to us Parkinson’s patients, and I relly think it will help us enjoy our lives even better. Now that is news to be hopeful for, huh?
So what are your thoughts? Am I completely nuts (don’t answer that), way off-base with this idea, wishy-washy, or right on? As usual, leave your comments below for all to ponder.
OK, my brain is tired after all that thinking – time for a nap! But I’ll be back with more DEEP BRAIN THOUGHTS so stay tuned!
![]()


